▎WuXi AppTec Content Team Editor
At present, atherosclerotic cardiovascular disease (ASCVD) has become the first cause of death among Chinese residents. Dyslipidemia is the main pathogenic risk factor in the development of ASCVD. The overall prevalence of dyslipidemia among Chinese adults is as high as 40.4%. Effective control of dyslipidemia is of great significance to the prevention and control of ASCVD. So how should different groups of people prevent and control dyslipidemia? Let’s take a look at this article today.
Image source: 123RF
Dyslipidemia, what indicators should I look for?
Blood lipids refer to the general term for cholesterol, triglycerides and lipids (such as phospholipids) in serum. Dyslipidemia usually refers to elevated serum cholesterol and/or triglyceride levels; also generally refers to includinghigh-density lipoprotein cholesterol (HDL-C) low levels of various dyslipidemia.
The basic items of clinical blood lipid testing are serum total cholesterol, triglyceride, low density lipoprotein cholesterol (LDL-C), HDL-C. The clinical application value of other blood lipid items such as Apolipoprotein A1 (Apo A1), Apo B, lipoprotein(a) [Lp(a)] has also attracted increasing attention. The current clinical ASCVD prevention and control pay close attention to cholesterol and triglycerides.
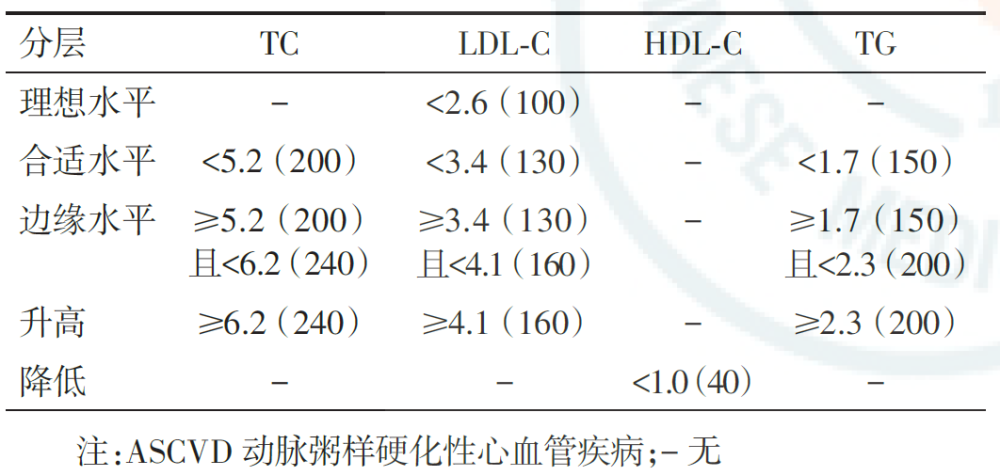
▲Appropriate levels of blood lipids and abnormal stratification criteria for primary prevention of ASCVD in China (mmol/L) (Image source: Reference [2])
What are the dangers of dyslipidemia?
Dyslipidemia characterized by elevated LDL-C or triglycerides is an important risk factor for ASCVD, the higher the LDL-C, the higher the risk of ASCVD The higher the triglyceride level, the risk of ASCVD is increased, and its severe increase also increases the risk of acute pancreatitis.
General principles of dyslipidemia treatment
Dyslipidemia is obviously affected by diet and lifestyle, and must control diet and improve lifestyle regardless of drug treatment.
According to the different risk levels of individual ASCVD(can be divided into very high risk, high risk, intermediate risk, low risk), determine lipid regulation The basic target value of cholesterol that treatment needs to achieve.
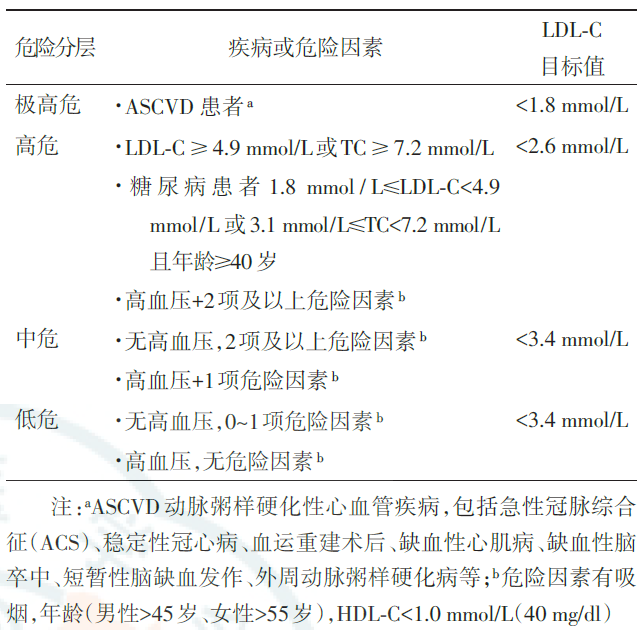
▲Dyslipidemia risk stratification and target value (Image source: Reference [2])
Global guidelines for the prevention and treatment of dyslipidemia all emphasize that LDL-C plays a central role in the pathogenesis of ASCVD, and LDL-C is recommended as the primary intervention target, andnon-HDL-C is recommended. -C may serve as a secondary intervention target.
Lipid-lowering therapy needs to set target values: LDL-C < 1.8 mmol/L in very high risk patients, LDL-C < 2.6 mmol/L in high risk patients, moderate LDL-C <3.4 mmol/L in high-risk and low-risk patients.
The baseline LDL-C value is high, and if the target value cannot be reached, the LDL-C should be reduced by at least 50%. For very high-risk patients whose LDL-C baseline is within the target value, LDL-C should still be reduced by about 30%.
Lipid-lowering drugs mainly include statins, cholesterol absorption inhibitors, fibrates, high-purity fish oil preparations, PCSK9 inhibitors, etc.
Statins significantly reduce the risk of cardiovascular events in both primary and secondary prevention of ASCVD. Therefore, in order to reach the lipid-lowering target of LDL-C, statin lipid-lowering drugs should be the first choice in clinical practice. A moderate-intensity statin should be used initially, and the dose should be adjusted appropriately according to the individual’s cholesterol-lowering efficacy and tolerance.
If triglycerides are only mildly to moderately elevated (2.3 mmol/L~5.6 mmol/L), in order to prevent and control ASCVD, although the main goal is to reduce the level of LDL-C, it should be emphasized that non-HDL-C needs to reach the basic target value. After statin treatment, if non-HDL-C still cannot reach the target value, fibrates and high-purity fish oil preparations can be added on the basis of statins. For patients with severe hypertriglyceridemia, that is, fasting ≥5.7 mmol/L, the use of drugs that mainly lower triglycerides and very low-density lipoprotein cholesterol (VLDL-C) should be considered first, such as strong>Fibrates, high-purity fish oil preparations, or niacin.
How to manage dyslipidemia in different populations?
Hypertriglyceridemia
In addition to intensive lifestyle interventions, triglyceride-lowering therapy should be initiated in the following situations:
1) When triglyceride ≥5.6 mmol/L, acute pancreatitis needs to be prevented.
2) Patients at high risk of cardiovascular disease (such as diabetic patients) who have reached the LDL-C target but still have triglycerides ≥2.3 mmol/L, primary prevention of ASCVD is required .
3) ASCVD patients who have reached the LDL-C target but still have triglycerides ≥2.3 mmol/L, secondary prevention of ASCVD is required.
China has a high prevalence of hypertriglyceridemia. Triglyceride-lowering drugs are fibrates or high-purity fish oil, and should be monitored during treatment Safety indicators, making non-HDL-C reach the target (LDL-C target value + 0.8 mmol/L).
Hypertension with dyslipidemia
1) All hypertensive patients with high risk, very high risk and super high risk of ASCVD, must start antihypertensive combined with LDL-C lowering drug therapy at the same time.
2) Hypertensive patients with intermediate-risk ASCVD, if <55 years old, should be assessed for cardiovascular risk for the rest of their life. For those with high-risk ASCVD or with LDL-C≥2.6 mmol/L, strong>At the same time of lifestyle intervention, LDL-C lowering drug therapy can be considered.
3) Hypertensive patients with low-risk ASCVD should undergo non-drug (lifestyle) intervention for 3 to 6 months. If LDL-C is below the target level, non-drug therapy can be continued intervention. For those who cannot reach the LDL-C target after non-drug therapy, additional moderate-intensity statin therapy can be considered.
In Chinese hypertensive patients, 41.3% had dyslipidemia. The awareness rate, treatment rate and control rate of dyslipidemia in Chinese hypertensive patients are quite unsatisfactory. Therefore, attention should be paid to the management of dyslipidemia in hypertensive patients.
Diabetes with dyslipidemia
The serum LDL-C level of diabetic patients aged ≥40 years should be controlled below 2.6 mmol/L, and the target HDL-C value should be kept above 1.0 mmol/L. According to the characteristics of dyslipidemia, statin therapy is the first choice. For patients with high triglycerides with or without low HDL-C, the combination of statins and fibrates can be used.
Patients with type 2 diabetes have dyslipidemia, which further increases the risk of macrovascular and microvascular complications. Chinese patients with type 2 diabetes have a high proportion of dyslipidemia, and the treatment rate and compliance rate are low. The CCMR-3B study investigated 25,817 outpatients with type 2 diabetes in 104 hospitals in China, and found that 42% of type 2 diabetes patients had dyslipidemia, of which only >55% of patients received lipid-lowering therapy. In addition, only 12% of patients in this study reached the standard of serum total cholesterol, triglyceride, LDL-C, and HDL-C. This suggests that the management of blood lipids in patients with type 2 diabetes should be strengthened clinically.
Senior elderly with dyslipidemia
1) Non-drug treatment: Elderly patients over 75 years old should consume unsaturated fatty acids on the basis of ensuring caloric intake, Aggressive exercise weight loss is not recommended as routine treatment.
2) Drug treatment: Elderly people aged ≥80 years often suffer from a variety of chronic diseases, requiring multiple drugs, and most of them have varying degrees of Liver and kidney function decline, older clinical ASCVD patients can start statin therapy after evaluating adverse reactions, drug interactions, physical weakness and preferences. The selection of lipid-lowering drug dose needs to be individualized, and the initial dose should not be too large. The dose of lipid-lowering drug should be adjusted according to the therapeutic effect, and liver and kidney functions and creatine kinase should be closely monitored.
Existing studies have shown that elderly patients with hypercholesterolemia and cardiovascular disease or diabetes may benefit from lipid-lowering therapy.
Ischemic stroke with dyslipidemia
Patients with non-cardiac ischemic stroke should first consider medium and high-intensity statin therapy, and adjust the dose appropriately according to individual lipid-lowering efficacy and tolerance; Very high risk ischemic stroke patients, if LDL-C ≥ 1.8 mmol/L after statin therapy, combined PCSK9 inhibitor or ezetimibe therapy is recommended; For patients with ultra-high risk ischemic stroke, it is recommended to directly initiate statin and PCSK9 inhibitor combination therapy.
China’s ischemic stroke mortality and morbidity have been increasing year by yearUpward trend. LDL-C is an independent risk factor for ischemic stroke. On the basis of standardizing the secondary prevention of stroke, further strengthening lipid-lowering has clinical significance for preventing the recurrence of stroke.
Non-cardiac ischemic stroke patients belong to very high-risk patients, and the lipid-lowering target value is LDL-C<1.8 mmol/L and is higher than the baseline. Level reduction ≥50%; if any of the following conditions exist: history of previous stroke, intracranial artery stenosis ≥70% or carotid artery stenosis ≥50%, after carotid endarterectomy/stent angioplasty, Coronary heart disease, peripheral arterial disease, and diabetes mellitus meet the criteria for ultra-high-risk patients, and the lipid-lowering target value is LDL-C < 1.4 mmol/L, with a decrease of ≥50% compared with the baseline level.
Familial Hypercholesterolemia (FH)
The treatment of FH begins with maintaining a healthy lifestyle; while also emphasizing prevention and control of other coexisting risk factors, such as hypertension and diabetes. Second, FH patients start statin therapy from adolescents (age >10 years old), and need long-term adherence to reduce the risk of ASCVD.
Malignant tumor patients with dyslipidemia
For the treatment of dyslipidemia in tumor patients, patients whose blood lipids cannot reach the target by lifestyle adjustment need to start lipid-lowering drug therapy. Lipid-regulating drugs mainly include statins and fibrates.
Abnormal lipid metabolism is not only closely related to the occurrence of cardiovascular diseases, but also closely related to the occurrence, development, invasion and metastasis of tumors (such as breast cancer, ovarian cancer, endometrial cancer, etc.) .
Finally, In the past 30 years, the blood lipid level of the Chinese population has gradually increased, and the prevalence of dyslipidemia has increased significantly. Effective control of dyslipidemia is of great significance to the prevention and control of ASCVD. Adjusting the dietary structure and adopting a healthy lifestyle are the basic strategies for preventing and treating dyslipidemia. In addition, in terms of drug treatment, different types of patients should choose appropriate lipid-lowering drugs for treatment according to their own conditions.