This article was written by Karl
For a long time, colleagues in thyroid and breast surgery have found that more and more patients with early-stage thyroid cancer are being admitted.
The diagnosis of “thyroid nodule” is appearing on more and more people’s medical reports. Even many patients with nodules smaller than 1 cm have a strong desire for biopsy. Most of the pathological results of fine needle aspiration biopsy are “papillary thyroid carcinoma” with a low degree of malignancy.
This clinical phenomenon is also consistent with the statistical results. A JAMA article mentioned that the incidence of thyroid cancer in the United States increased from 3.6 per 100,000 in 1973 to 8.7 per 100,000 in 2002—a 2.4-fold increase. But the incidence of follicular thyroid carcinoma, medullary carcinoma and anaplastic carcinoma did not change significantly.
That is, these increases are largely attributable to an increase in the incidence of papillary thyroid cancer, which increased from 2.7 to 7.7 per 100,000 people—a 2.9-fold increase. From 1988 to 2002, 49% of cancers that increased were smaller than 1 cm; 87% were smaller than 2 cm. [1]
Image source: Reference 1
The increased incidence of small tumors may be related to the popularity of ultrasound screening. However, if the increased incidence of small tumors was solely due to widespread screening, the incidence of larger tumors would decline in subsequent years due to prompt diagnosis and treatment, as many tumors develop when they are asymptomatic and small in size. will be detected and treated.
However, the reality is just the opposite, and the incidence of large tumors has also maintained a steady upward trend. [2]
10 million people die each year from cancer
From a causal logic, it may be more than just the detection rate that increases the incidence of cancer.
The year-over-year increase in data suggests that there are other risk factors contributing to the increased prevalence of thyroid cancer, perhaps more frequent nuclear medicine examinations leading to increased radiation exposure, or industrial Development has led to increased occupational exposure. [3]
In 2019, there were an estimated 23.6 million new cancer cases and 10 million cancer deaths globally, resulting in approximately 250 million disability adjusted life years (DALYs) . Since 2010, new cancer cases have increased by 26.3%, deaths have increased by 20.9%, and DALYs have increased by 16.0%.
More and more people are dying of cancer.
Cancer is currently the second leading cause of death and DALYs globally, after cardiovascular disease. In countries with high SDI (Socio-demographic Index), cancer has even surpassed cardiovascular disease as the number one cause of DALYs. [4]
A month ago, The Lancet published a survey entitled The global burden of cancer attributable to risk factors, 2010–19: a systematic analysis for the Global Burden of Disease Study 2019 The report analyzed cancer cases over the past 10 years. [5]

Image source: Lancet screenshot
GBD 2019 risk factors are divided into three groups: environmental and occupational, behavioral, and metabolic. The study included 82 cancer risk-outcome pairs (23 cancer types and 34 risk factors). Risk factor exposure levels and distributions were modeled for each age, sex, location, and year based on data provided by published studies, household surveys, censuses, administrative data, ground-based surveillance data, or remote sensing data.
Using estimates of cancer cases and deaths in more than 200 countries around the world, researchers found that in 2019, the 34 risk factors included in the analysis were responsible for 4.45 million deaths, It accounted for 44.4% of all cancer deaths, 50.6% among men and 36.3% among women. At the same time, these risk factors resulted in 105 million DALYs.
Nearly half of cancer deaths are preventable
Reportedly, a large portion of the global cancer burden, including nearly half of all cancer deaths, has the potential to be prevented through interventions.
For example, among these risk factors, the top three causes of death and DALYs are smoking, alcohol consumption, and being overweight (high BMI).
For global risk-attributable cancer DALYs for both men and women, the most important risk factor was smoking, which accounted for 33.9% of all male cancer DALYs in 2019, and all 10.7% of female cancer DALYs.
Smoking is associated with approximately 80 to 90 percent of lung cancer deaths in the United States. Smokers are less likely to develop or die from lung cancer than non-smokers15 to 30 times as much. Even smoking a few cigarettes a day or smoking occasionally increases your risk of lung cancer. The more cigarettes a person smokes per day and the number of years, the greater the risk.
In addition, smoking can cause cancer in almost any part of the body. Smoking causes cancer of the mouth and throat, esophagus, stomach, colon, rectum, liver, pancreas, larynx, trachea, bronchus, kidney and pelvis, bladder and cervix, acute myeloid leukemia . The accumulation of this series of tumor lists, coupled with the global prevalence of smoking culture, makes the harm of smoking to people around the world always high. [6]
Among men, alcohol use, dietary risk, and air pollution accounted for 7.4%, 5.9%, and 4.4% of all male cancer DALYs in 2019, respectively.
In women, unsafe sex was the second-leading risk factor, accounting for 8.2% of all female cancer DALYs in 2019, followed by dietary risk (5.1%), overweight (4.7%) ) and diabetes (3.6%).
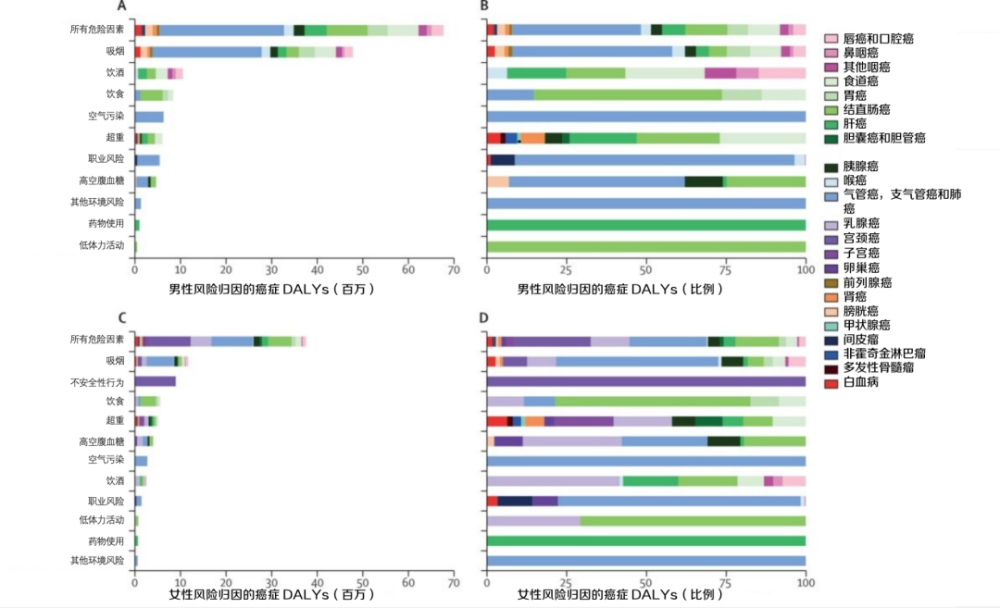
Image source: Reference 5
The global risk-attributable proportion of risk factors for cancer death is similar. The report argues that these factors are likely to be prevented through interventions.
Admission review for 3 days, relapse on the day of discharge?
“The Yellow Emperor’s Classic of Internal Medicine” mentions, “The superior doctor treats the disease before, the traditional Chinese medicine treats the disease of desire, and the inferior doctor treats the disease already.” It can be said that China had the concept of disease prevention more than 2,000 years ago. But in fact, even knowing the importance of prevention, everyone is still lucky.
Take smoking as an example, everyone’s understanding of the harm of smoking is probably like the phrase “smoking is harmful to health” printed on cigarette packs: I see it, but I don’t fully see it. Most people, even doctors, still need to smoke.
A 2004 census of 3,552 doctors from six cities in China showed that Chinese doctors, the people most aware of the dangers of tobacco in the country, had a smoking rate of 23%, of which 41% of men and 1% of women. [7]
“Cigarette delivery culture” is one of the objective reasons. Sometimes hiding in the corridor and smoking together in Lala’s home can indeed quickly shorten the distance with colleagues and superiors, and what’s more “Quitting alcohol is quitting friends.”
Of course, there are also subjective reasons. Survivorship bias is prone to exist when the problem of prevention is not directly causally related to the disease. “Smoked and drank everything, and lived to be 100 years old” is a classic case that many smokers and drinkers and even my colleagues like to talk about.
In addition, I want to talk about a more practical point: at the diagnosis and treatment level, doctors will be less involved and more difficult to prevent patients.
In cancer prevention, we usually pay more attention to secondary prevention measures such as cancer screening, while neglecting primary prevention related to personal behavior such as smoking and obesity. “Take care but neglect management”. Even in hospitals where smoking is prohibited, opening the toilet door can often lead to the pungent smell of smoke.
A colleague once shared with me a “new disease smoking cessation method” for an elderly patient with coronary heart disease: Review for 3 days after admission, and resume smoking on the day of discharge. After being asked and told seriously, the reply “I can’t help but smoke a few times, the disease has been cured anyway.”
Doctors share outpatient experience at Lilac Garden Forum
In fact, at the current stage of the development of modern medicine, “health concerns in out-of-hospital settings” cannot be ignored for a long time. In the past, the Chinese people’s health habit was “go to the hospital when you are sick”, and even many people “go to the hospital when they can’t hold it anymore”.
The story of the three Bian Que brothers was mentioned in He Guan Zi Shi Xian XVI. Bian Que said: “The eldest brother treats the disease as a spirit, but he does not have a form to get rid of it, so the name does not come from the family. The middle brother treats the disease, it is in the hair, so the name does not come from Lu. If you are a Bian Que, the blood is the blood. Poison, sub-skin, leisurely and famous among the princes.”
The patient longed for Bian Que, but the doctor wanted to be the eldest brother of Bian Que. (planner: carollero; producer: gyouza)
Acknowledgments: This article has been professionally reviewed by Wang Jinhu, Chief Physician of Oncology Surgery, Children’s Hospital Affiliated to Zhejiang University School of Medicine, and Ye Yao, Chief Physician of Colorectal Surgery, The Second Affiliated Hospital of Zhejiang University School of Medicine
Note
Ye Yao, attending physician of colorectal surgery affiliated to the Second Hospital of Zhejiang University School of Medicine, reviewed comments:
Although primary prevention of tumors seems to be able to greatly reduce the incidence of tumors, there are great difficulties in the development and promotion of primary prevention in clinical practice. For doctors, primary prevention not only requires doctors to invest time and energy in popularizing science, but also requires patients’ own compliance and long-term self-management, and also requires social promotion.
According to the results of this study, the majority of tumor burden cannot be avoided, even after controlling for risk factors. so primary preventionThere is no doubt about the need to push. But how to do this effectively is not just a medical problem, but a social one.
The source of the title map: Figure Worm Creative
References:
[1] Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006 May 10;295(18):2164-7. doi: 10.1001/jama.295.18.2164. PMID: 16684987.
[2] Li N, Du XL, Reitzel LR, Xu L, Sturgis EM. Impact of enhanced detection on the increase in thyroid cancer incidence in the United States: review of incidence trends by socioeconomic status within the surveillance, epidemiology, and end results registry, 1980-2008. Thyroid. 2013 Jan;23(1):103-10. doi: 10.1089/thy.2012.0392. PMID: 23043274; PMCID: PMC3539256.
[3] Cui Y, Mubarik S, Li R, Nawsherwan, Yu C. Trend dynamics of thyroid cancer incidence among China and the U.S. adult population from 1990 to 2017: a joinpoint and age- period-cohort analysis. BMC Public Health. 2021 Mar 31;21(1):624. doi: 10.1186/s12889-021-10635-w. PMID: 33789605; PMCID: PMC8010947.
[4] Global Burden of Disease 2019 Cancer Collaboration, Kocarnik JM, Compton K, et al. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022 Mar 1;8(3):420-444. doi: 10.1001/jamaoncol.2021.6987. PMID: 34967848; PMCID: PMC8719276.
[5] GBD 2019 Cancer Risk Factors Collaborators. The global burden of cancer attributable to risk factors, 2010-19: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2022 Aug 20;400(10352):563-591. doi: 10.1016/S0140-6736(22)01438-6. PMID: 35988567; PMCID: PMC9395583.
[6]https:https://www.cdc.gov/cancer/lung/basic_info/risk_factors.htm#:~:text=People%20who%20smoke%20cigarettes%20are, the%20risk%20of%20lung%20cancer.
[7] Jiang Y, Ong MK, Tong EK, Yang Y, Nan Y, Gan Q, Hu TW. Chinese physicians and their smoking knowledge, attitudes, and practices. Am J Prev Med . 2007 Jul;33(1):15-22. doi: 10.1016/j.amepre.2007.02.037. PMID: 17572306; PMCID: PMC2800817.
Lilac Garden is a professional platform for medical practitioners, with the mission of “helping Chinese doctors”. Download the “Lilac Garden App” to discuss cases with peers, study open classes online, use clinical decision-making tools such as medication assistants, and find reliable medical positions in Lilac Talents.