1
First admission
October 28, 2020 – December 2, 2020
A 7-year-old boy was hospitalized with “intermittent fever for 7 days and disturbance of consciousness for 1 day”. After admission, the child developed convulsions, and the disturbance of consciousness worsened to coma. There was no personal or family history. special.
Auxiliary examination:
Cerebrospinal fluid (CSF) examination showed a white blood cell count of 84 × 10^6/L, normal biochemistry, and CSF herpes simplex virus (HSV) type 1 DNA positive;
Serum and cerebrospinal fluid autoimmune encephalitis-related antibodies were negative for 6 items; brain magnetic resonance (MRI) showed swelling of bilateral cerebral hemispheres and thalamus;
video-electroencephalography (VEEG) showed a background of diffuse slow waves, a large number of multifocal sharp waves, sharp slow waves, prominent right frontal area, and periodic discharge; diagnosis For herpes simplex encephalitis (HSE).
Acyclovir, intravenous injection of human immune globulin (IVIG), intravenous methylprednisolone and symptomatic and supportive treatment were given for 35 days. The patient was discharged from the hospital. At the time of discharge, the child was able to walk independently. Communicate normally with people.
2
Readmission
December 7, 2020
5 days after discharge, the patient gradually developed symptoms such as beating, scratching hair, involuntary movements of hands, perioral automatism with salivation, and sleep disturbance.
Auxiliary examination:
CSF routine and biochemical examination were normal, and CSF herpes simplex virus (HSV) type 1 DNA was negative;
Re-examination of 6 autoimmune encephalitis-related antibodies in serum and cerebrospinal fluid indicated that serum anti-NMDAR antibody IgG was 1:32, and CSF anti-NMDAR antibody IgG was 1:10;
Cranial MRI showed scattered patchy, slightly longer T1 and slightly longer T2, FLAIR high-intensity foci in bilateral cerebral hemispheres and thalamus, and the lesions improved with local atrophy;
Re-examination of VEEG showed multiple multifocal slow waves of medium and high amplitude, sharp-type slow waves, and slightly more delta brushing paroxysms in the left frontal and central areas during sleep; diagnosis of HSE secondary to anti-NMDAR encephalitis .
The IVIG and intravenous methylprednisolone pulse therapy were given again. After 2 weeks, the symptoms did not improve. Cyclophosphamide pulse therapy was added once a month. The symptoms of the child recovered after 2 months. normal. Cyclophosphamide treatment was continued once a month for a total of 6 times; at the same time, oral prednisone was gradually reduced, and the total course of treatment was stopped for 1 year.
Up to now, the child has no neurological symptoms and positive signs.
https://https://https://https:///
The child had symptoms such as abnormal mental behavior and sleep disturbance soon after herpes simplex encephalitis improved and was discharged from the hospital. The final diagnosis was herpes simplex encephalitis secondary to anti-NMDAR encephalitis. inflammation. So what kind of disease is anti-NMDAR encephalitis? How to identify? How to treat it?
3
Anti-NMDAR Encephalitis
Autoimmune encephalitis (AE) is an inflammatory disease of the central nervous system caused by an autoimmune reaction. The main clinical features include acute or subacute seizures, cognitive Disorders and psychiatric disorders.
The most common clinical type is anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis. [1]
1. Clinical manifestations
80% of patients with anti-NMDAR encephalitis have prodromal symptoms such as fever, headache, vomiting, and diarrhea, often lasting 5 to 14 days. [2]
According to the progression of the disease, it can be divided into 5 stages, namely the prodromal stage, the psychotic symptom stage, the involuntary movement stage, the non-responsive stage, and the recovery stage. There is no strict demarcation between the stages. [3]
Core symptoms include [3, 4]:
(1) Prominent mental and behavioral abnormalities or cognitive dysfunction: anxiety, agitation, bizarre behavior, hallucinations, delusions, disordered thinking, psychotic symptoms. Cognitive dysfunction can manifest as memory loss.
(2)Language dysfunction: continuous uninterrupted compulsive speech, dysarthria, speech reduction, mutism, imitation speech, etc.
(3) Seizures are of various forms, with focal seizures more common, and status epilepticus may occur in severe cases. Generally, there are no “generalized seizures” such as myoclonic seizures, absence seizures, and myoclonic-atonic seizures.
(4)Frequent movement disorders: orofacial movement disorders, choreoathetosis-like movements, dystonia, rigidity, opisthotonous postures.
(5) The level of consciousness decreases, the response to stimuli is weakened, and it also alternates with states of tension and anxiety. Patients are generally in the “three no states”, that is, “no eating, moving, and no speech”, accompanied by a lot of salivation.
(6) Autonomic instability: hyperthermia, blood pressure fluctuations, tachycardia, bradycardia, apnea, and sometimes hypoventilation requiring mechanical ventilation.
Mental behavior abnormalities, seizures, and movement disorders/involuntary movements are the common first symptoms of anti-NMDAR encephalitis, and the incidence is related to the age of onset. Children under 12 years old Half started with seizures or dyskinesia/involuntary movements.
2. Auxiliary Exams
(1) Cerebrospinal fluid (CSF): The white blood cell count is slightly elevated or normal, mainly monocytes. The cerebrospinal fluid protein is normal or slightly elevated, and the oligoclonal zone may be positive. The positive cerebrospinal fluid anti-NMDAR antibody is a necessary condition for the diagnosis of anti-NMDAR encephalitis.
(2) Cranial MRI: no specific manifestations, can involve multiple parts, such as cortex, white matter, hippocampus, cerebellum, basal ganglia, etc. T1, long T2 signal, FLAIR high signal.
(3) EEG: can be manifested as diffuse or focal slow waves, epileptiform discharges, extreme delta brushing, etc.
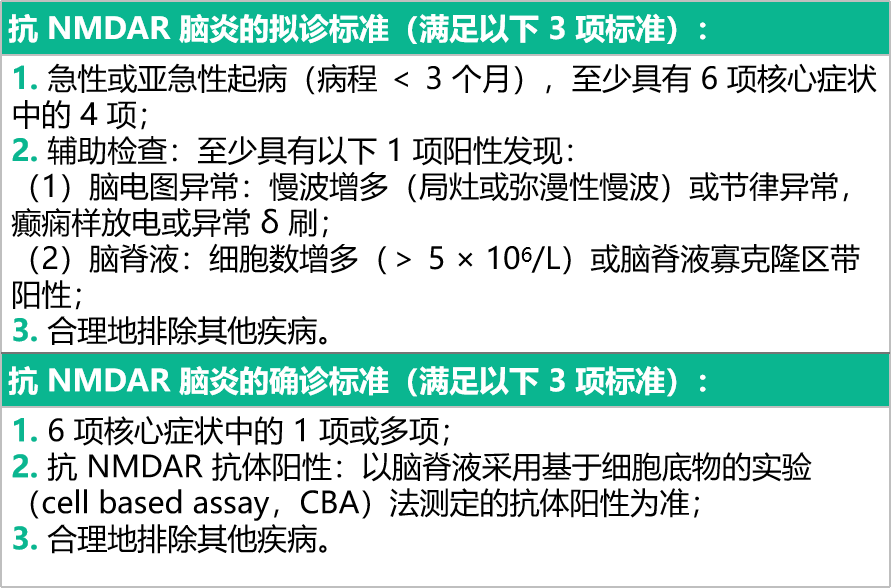
3. Diagnostic criteria[5]
4. Differential Diagnosis
Other types of autoimmune diseases, primary mental disorders (acute psychosis or schizophrenia), malignant catatonia, viral encephalitis, encephalitis lethargica, etc.
5. Treatment
There is no standard treatment for this condition in children. The expert consensus on diagnosis and treatment of autoimmune encephalitis in China (2017) mentioned that the treatment of this disease includes immunotherapy, tumor treatment, control of epilepsy symptoms and control of psychiatric symptoms.
(1)Immunotherapy
Includes first-line immunotherapy, second-line immunotherapy, and long-term immunotherapy.
First-line immunotherapy includes corticosteroids, intravenous human immunoglobulin, and plasma exchange.
Second-line immunotherapy, including rituximab and intravenous cyclophosphate, is mainly used for patients who have not responded well to first-line immunotherapy.
Long-course immunotherapy drugs, including mycophenolate mofetil and azathioprine, are mainly used in recurrent cases, but also in patients with poor response to first-line immunotherapy and tumor-negative anti-NMDAR brain tumors. inflammation patients.
(2)Treatment of tumors
Anti-NMDAR encephalitis can be associated with ovarian teratoma and should be removed as soon as it is detected. For female patients ≥ 12 years of age with no tumor found, pelvic ultrasonography every 6 to 12 months for 4 years after illness is recommended.
(3)Control of epilepsy symptoms
Since epilepsy symptoms are caused by an autoimmune reaction, antiepileptic drugs are generally less effective. Broad-spectrum antiepileptic drugs, such as benzodiazepines, sodium valproate, levetiracetam, and lamotrigine, can be used.
(4)Control of psychiatric symptoms
Olanzapine, clonazepam, sodium valproate, haloperidol, and quetiapine are among the options available.
Summary
Anti-NMDAR encephalitis is a well-characterized autoimmune encephalitis characterized by prominent psychiatric and cognitive impairment, speech impairment, seizures, dyskinesia, and other motor deficits Abnormalities, decreased level of consciousness, and autonomic instability. Early treatment can improve outcomes, speed up recovery, and reduce the risk of recurrence.
Planning: Zhang Jie
Title image: Zhanku Hailuo
1. Hu Yamei, Jiang Zaifang, Shen Kunling, Shen Ying. Zhu Futang Practical Pediatrics (8th Edition) [M]. People’s Health Publishing House. 2015.
2. Ma Jiannan, Jiang Li. The etiology and pathogenic mechanism of autoimmune encephalitis [J]. Chinese Journal of Practical Pediatrics, 2019, 34(24):5.
3. Ji Taoyun, Jiang Yuwu. Early diagnosis of autoimmune encephalitis [J]. Chinese Journal of Practical Pediatrics, 2019, 34(24):4.
4. Josep Dalmau, MD, PhD, Myrna R Rosenfeld, MD, PhD. Paraneoplastic and Autoimmune Encephalitis. UpToDate Clinical Consultant. (Accessed on Jul 08, 2022).
5. Prüss H, Dalmau J, Harms L, et al. Retrospective analysis of NMDA receptor antibodies in encephalitis of unknown origin. Neurology. 2010;75(19):1735-1739. doi :10.1212/WNL.0b013e3181fc2a06
6. Neurology Branch of Chinese Medical Association. Expert consensus on diagnosis and treatment of autoimmune encephalitis in China [J] . Chinese Journal of Neurology, 2017, 50 (2): 91-98.
p>