Friday, a hernia operation was underway.
Dr. Zhang, who was under anesthesia, looked at the monitor with a solemn expression. The surgeon on the operating table, seeing that Dr. Zhang seemed serious, did not forget to make a joke to break the atmosphere.
However, a few flirtatious remarks failed to get Dr. Zhang to look at him.

The doctor on stage thought: What about a hernia operation? Besides, the patient’s condition is very good, and it is not the old, the weak, the sick or the disabled. Although this patient is in his 60s, he has cultivated more than ten acres of land.
Yes, the old man lying on the operating table is indeed very strong. Whoever said on the Internet that the body fat rate is low, this old man is not inferior. Moreover, this tendon meat can work.
Then here comes the question: Why is the anesthesiologist nervous because the old man is so healthy?
What Dr. Zhang saw was an unusual problem. He said afterwards: This is the first case he has encountered in recent years. The last case was a few years ago.
In the operating room, everyone is afraid that the anesthesiologist will be busy. If the anesthesiologist chatted with everyone leisurely there, or even looked at the mobile phone, everyone would not be surprised. But if the anesthesiologist gets busy, everyone gets nervous. This is because the primary task of an anesthesiologist in the operating room is the safety of the patient. Anesthesiologists are busy and patients may be at risk.

Dr. Zhang at this time was not busy, nor could he be busy. Because he didn’t know what happened to the patient. In my brain, I was quickly thinking about why.
Although almost everyone shy away from thinking about the worst, the profession of anesthesiologist is to list the most serious risks first.
Dr. Zhang thought: Could it be malignant hyperthermia? If so, that’s too dangerous. This danger may only be experienced by experienced anesthesiologists. Unconsciously, Dr. Zhang glanced at the old man lying on the operating table. In my heart, I couldn’t help worrying about the old man. He knew that if it was a vicious high fever, he was not fully sure of saving him.
On the operating table, only the assistant noticed everything under the table. Others, concentrate on laparoscopic hernia repair.
At this point, the end of exhalation is over 50. This kind of value, the machine must be alarmed. Although the body temperature has been stable at 36 degrees, Dr. Zhang still pressed the mute button again and again, and he did not dare to easily rule out malignant hyperthermia. He knows that if the problem is simple, it may lead to insufficient rescue preparations later.
What calms his nervousness a bit is that as time goes by and the end-expiratory value exceeds 60, his body temperature remains stable.
Some people say, why not deal with such a high end-expiratory value?

He certainly handled it! Quietly, he has increased the flow of fresh gas and increased tidal volume. Even, the first time he noticed the abnormality, he stopped the inhalation anesthetic according to the malignant hyperthermia standard. Another advantage of a large flow of fresh gas is to accelerate the discharge of carbon dioxide.
However, despite all that has been done, the end-expiratory value is only temporarily stuck in the 50s. Although he was calm on the surface, he was also panicked inside. However, he couldn’t let others see it. The anesthesiologists were panicking, so they couldn’t play.
Although he was nervous, his knowledge told him that although malignant hyperthermia could not be ruled out, there were various indications that this scary situation originated from the operation of the doctor on the operating table. Because, at this time, it is laparoscopic hernia repair.
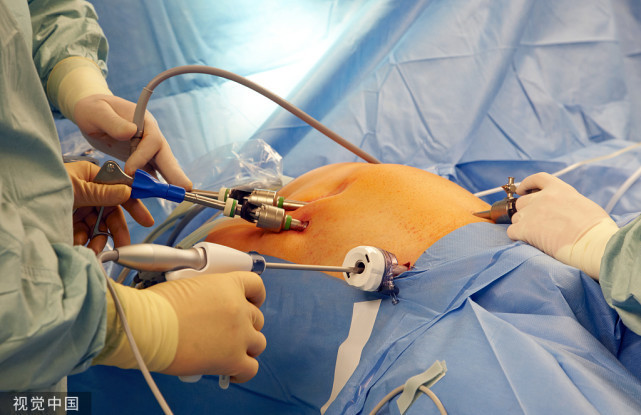
During the repair procedure, the covering of the hernia is swum away and a patch is placed inside. In the absence of a complete membrane, the carbon dioxide filling the abdominal cavity may diffuse into loose tissue or other cavities, or even overflow into the subcutaneous tissue.
However, reaching out and pinching the patient’s chest subcutaneously, no abnormality was found. However, he could not be reassured.
Finally, after another 20 minutes of suffering, he finally felt a “snow grip” under the skin of the patient’s chest.
Although the patient’s end-tidal carbon dioxide was still at more than 50 at this time, Dr. Zhang’s heart was almost overjoyed. He knew that the patient was not malignant hyperthermia. The cause of the problem lies in the carbon dioxide gas used in laparoscopy to create a pneumoperitoneum.
With a clear direction, Dr. Zhang further adjusted the breathing parameters, and the normal atmosphere in the operating room was restored.
[Warm reminder] Please pay attention, here are a lot of professional medical science, to reveal the secrets of surgical anesthesia for you~