▎WuXi AppTec Content Team Editor
Current clinical practice guidelines recommend the use of high-intensity statins for robust LDL-C reduction in patients with established atherosclerotic cardiovascular disease (ASCVD). However, there is also a lot of evidence that, compared with increasing the dose of a single lipid-lowering drug, the combined use of lipid-lowering drugs can achieve a more significant effect and further reduce the risk of cardiovascular events.
Ezetimibe can effectively inhibit the absorption of cholesterol in the intestine, thereby reducing the transport of cholesterol to the liver and lowering the level of cholesterol in the blood. The addition of ezetimibe to lower-intensity statins may provide a viable alternative treatment strategy compared to high-intensity statins alone. Recently, The Lancet (THELANCET) published blockbuster research results, confirmed that moderate-intensity statin combined with ezetimibe has a lipid-lowering effect that is not inferior to high-intensity statin monotherapy.
Patients in the study who received a combination of moderate-intensity statins and ezetimibe not only had a lower 3-year risk of composite cardiovascular events, but also achieved LDL-C lipid lowering The proportion of targets was also significantly higher. For patients with a higher risk of statin side effects, or those with intolerance to high-intensity statin therapy, combination therapy may be considered as early as possible. The paper emphasizes that Based on the results of this study, the blood lipid management model is expected to usher in an important change in concept, and the future combination therapy is expected to become the initial choice of lipid-lowering therapy for high-risk patients with cardiovascular disease!

Screenshot source: THE LANCET
Meta-analyses of multiple randomized clinical trials show that lower-intensity statins combined with ezetimibe are expected to significantly reduce LDL compared with high-intensity statin monotherapy At the same time, reduce the dose of statin drugs, so as to avoid the occurrence of adverse events under high-intensity statin therapy and the potential statin intolerance of patients. However, so far, there is no randomized clinical trial comparing the long-term clinical outcomes of these two treatment strategies in ASCVD patients.
The current trial, called RACING, compared moderate-intensity statin + ezetimibe therapy in high-risk patients “ and “high-intensity statin monotherapy”‘s 3-year clinical efficacy and safety data to evaluate whether the combined strategy of statin + ezetimibe is effective in lowering cholesterol therapy.
The RACING trial is a multicenter, randomized, open-label, non-inferiority clinical trial that enrolled 26 South Korean patients between February 14, 2017, and December 18, 2018 There were 3780 patients with ASCVD at the medical center (75% male; mean age of all patients was 64 years). The median follow-up time of the study was 3 years.
Patients were randomly assigned in a 1:1 ratio to receive moderate-intensity statins combined with ezetimibe (1894 patients, rosuvastatin 10 mg + ezetimibe 10 mg, daily once orally) or high-intensity statin monotherapy (1886 patients, rosuvastatin 20 mg orally once a day).
Analysis of data showed: 40% of patients included in the study had a prior myocardial infarction (MI), 66% had undergone percutaneous coronary intervention (PCI), and 38% had diabetes.
The primary endpoint of the study was a 3-year composite of cardiovascular death, major cardiovascular events, and non-fatal stroke events in the ITT (intention-to-treat) population (non-fatal stroke) The inferiority margin was 2.0%). The data showed that a total of 172 patients (9.1%) in the combination therapy group had the primary endpoint event, and a total of 186 patients (9.9%) in the high-intensity statin monotherapy group had the primary endpoint event (absolute difference -0.78%; 90%). CI-2.39-0.83), post hoc analysis data confirmed that the study met the prespecified non-inferiority endpoint.
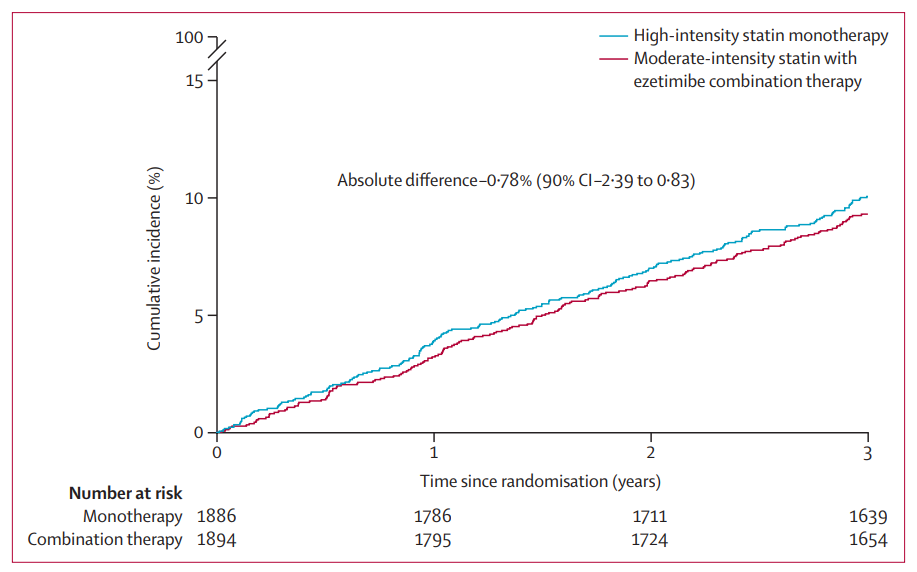
▲ITT population primary endpoint analysis results (Image source: Reference[1]) p>
Additionally, LDL-C levels were less than 70 mg/dL at 1, 2, and 3 years in the combination therapy group (70 mg/dL is usually a lipid-lowering target for high-risk patients) 73%, 75%, and 72% in the high-intensity statin monotherapy group, respectively, and 55%, 60%, and 58% in the high-intensity statin monotherapy group (both p values
Post hoc analysis of study data showed LDL-C levels below 55 mg/dL at 1, 2, and 3 years in the combination therapy group (55 mg/dL is usually extremely The proportions of patients with lipid lowering targets in high-risk patients) were 42%, 45%, and 42%, respectively, compared with 25%, 29%, and 25%, respectively, in the high-intensity statin monotherapy group. The median LDL-C level in the combination therapy group during the study period was 58 mg/dL, compared with 66 mg/dL in the high-intensity statin monotherapy group, which was significantly lower in the combination therapy group (p
In terms of safety, 88 (4.8%) and 150 (8.2%) patients in the combination therapy group and high-intensity statin monotherapy group discontinued or discontinued due to tolerance problems, respectively. The proportion of patients who discontinued or reduced the drug dose in the combination treatment group was significantly lower (p
Overall, the results of the current study support the addition of ezetimibe to combined lipid-lowering therapy in patients who are well-tolerated to moderate-intensity statin therapy. For patients at high risk of ASCVD-related events, the combination of moderate-intensity statins and ezetimibe was non-inferior to high-intensity statin monotherapy in the 3-year composite outcome, combination The treatment group not only had a higher proportion of patients with LDL-C levels below 70 mg/dL, but also had a lower incidence of drug discontinuation or dose reduction related to tolerance.
In general, older age, female gender, obesity, diabetes, hypothyroidism, chronic liver disease, and renal failure were significantly associated with statin intolerance. The results of the current study also suggest that patients with a higher risk of statin side effects, or those with intolerance to high-intensity statin therapy, may be considered for combination therapy as early as possible.